
Is Uganda’s CES the new face of resilient health systems in COVID?

Gloria Seruwagi
- January 4, 2021
As Uganda “peaks” on the COVID-19 trajectory with increasing cases from community transmission, the role of community leaders (political, cultural, and religious and others like VHTs and youth leaders) is more important than ever. Community-led interventions are very vital for acceptability and sustainability since the community better understands what suits them, and what behavioural change adjustments are feasible in the COVID-19 era. We see where the Ministry of Health is coming from, saying that “now is the worst time to get infected because our health system is constrained”. The Ministry is only echoing what the rest of the world’s leaders are appealing to their citizens about – in the UK, for example, the slogan is pretty much the same “stay home and protect the NHS”.
It is essential to foster resilient health systems; including and especially those at the grassroots. All of us need to be responsible and supportive of the national health system – in light of limited resources. There is so much to say about failure at the central level; however, with all the related inconveniences and frustrations associated with the plea to stay safe and out of hospital, the silver lining is that something revolutionary is happening – atleast in Uganda: we are invoking the power of prevention and critical place of grassroot stakeholders as high leverage intervention points. We are going back to the basics of public health and community protection. We are handing back power (despite the circumstances!) to the people to take charge of their health and its governance. What do you do when you feel “uncovered and exposed” by a system that’s supposed to protect you? A sane person will step up. A rational person will take charge and stop looking for solutions from the outside. And if different people, one by one, start doing this, then we are building critical mass and will eventually get to the place where our health really is in our hands. And prevention will lead the way – saving a whole lot of individual, household and national resources to tackle disease and death. We are the change we seek.
By taking this approach we are also dealing with also social accountability and addressing the demand side of healthcare, balancing the rights and responsibilities of health service users. The demand side is exactly that – always demanding for more, better and responsive services. And rightfully so. But we are trying to change this from being mostly demanding and highly dependent to being more proactive, responsible and supportive of our currently fragile health system. And strengthening ourselves, the “community”, as the first line of defense from disease and death. We define our own risk profile. We create our own narrative and identify the required solutions. We support those who are genuinely trying their best to provide essential quality care and services. And we demonstrate the irrelevance of those who have been poor stewards of population health. We draw the line. We strengthen the health system at individual, household and community level. We support the leaders, systems and structures at the level closest and truest to us – our VHTs and other critical community level stakeholders like our religious and cultural leaders, or youth representatives (the unsung heroes!). We rise and save our own lives.
The dynamic of this pandemic is a precursor to general health – that we cannot, and should never, fully rely on the facility health system; instead we should leverage local cohesion and the community being proactive about their health as a core responsibility. Community is the first and now last line of defense against COVID-19, so the timing is critical. And that time is now. Community is the one level where you invest so little but reap massive returns on investment. You put in so little but gain so much – most times instantly! Despite the dark times in which we currently live, I choose to remain optimistic. I remain hopeful and supportive of this intersecting point – the government’s Community Engagement Strategy (CES) of October 2020. It promises to invest in community and positions community at the forefront of responding to COVID-19. It is a super smart strategy with limitless potential for impact. Let’s hope that the necessary investment is expeditiously made to activate and fully operationalise it. With the CES resilience can be built and everybody wins – against COVID or anything that will ever be thrown our way.
About the Author
Gloria is a policy/systems researcher leading different COVID-19 studies in Uganda. She can be reached on gseruwagi@musph.ac.ug

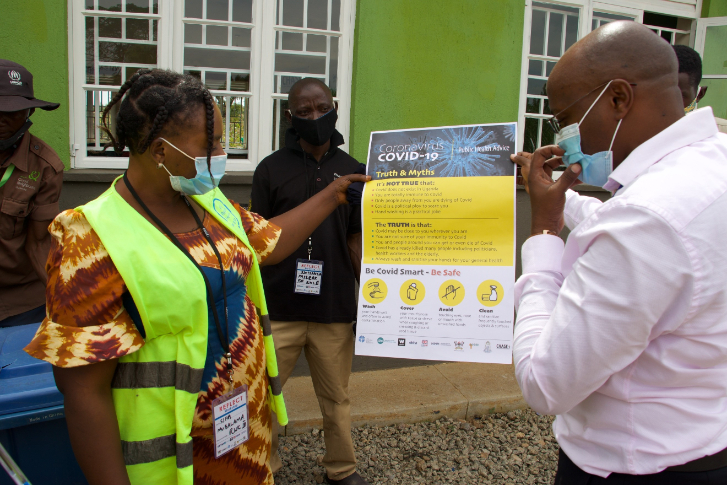
The writer (3rd left) with REFLECT study team members, ACORD field staff and a local private sector representative in Kyegegwa district

REFLECT study team members demonstrate proper facemask wearing to community leaders in Kyaka II Refugee Settlement, Uganda
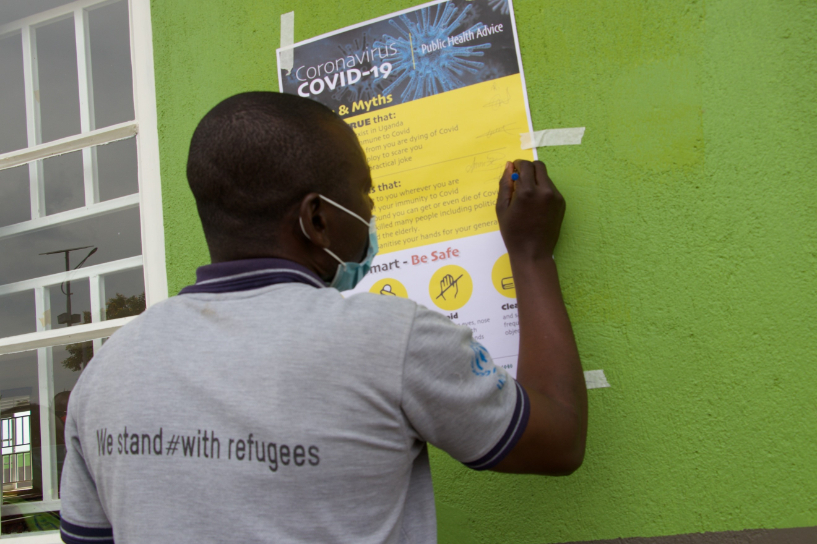
Above: Refugee community leaders prepare to pin up BCC materials on COVID-19 management; and
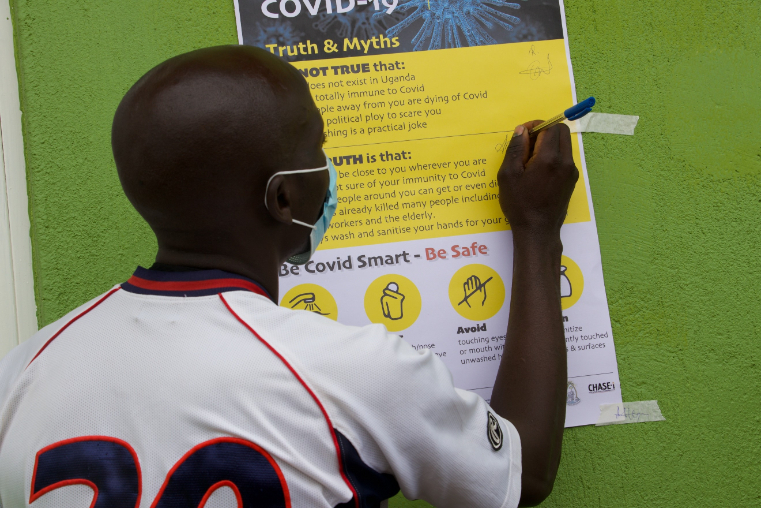
Below: Signing on a declaration to support an active COVID response in their communities

Above: Community leaders at the ALERTs study Validation and Co-Design Workshop on COVID-19 in Kampala slums;
Below: REFLECT study PI engaging community on a radio talkshow with the Head of Uganda national COVID Taskforce and the Disease Surveillance Lead from Kyegegwa District Local Government”

